



by Mary Ann Liebert: Severe acute respiratory syndrome coronavirus 2, known colloquially as COVID-19, was first identified in Wuhan, China, in December of 2019…
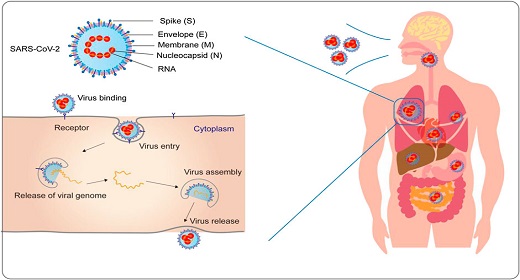
This novel coronavirus is known to be highly contagious with >4 million confirmed infections to date with a 6.9% mortality rate.1 There is no confirmed treatment or vaccine at the time of this writing. Supportive treatment is currently being employed for symptoms with the most common symptoms being fever, chills, shortness of breath, myalgias, headache, anosmia, dysgeusia, cough, and sore throat.
Acupuncture and other modalities of Chinese medicine have been underutilized/underreported in the United States, compared with China for the treatment of COVID-19. In response to a call by the Chinese government to employ Traditional Chinese Medicine (TCM) to help with prevention, treatment, and rehabilitation, the China Association of Acupuncture-Moxibustion developed guidance for acupuncture and moxibustion intervention on COVID-19. This guidance included advice on how to self-administer acupuncture and moxibustion under the direction of a physician in the various stages of disease process and recovery.2 China has reported that, as of February 17, 2020, about 85% of confirmed COVID-19 patients have been treated with TCM.3
This case report, with written HIPAA authorization obtained from the patient, is a description of a frontline anesthesiologist and medical acupuncturist with pulmonary symptoms likely consistent with severe COVID pneumonia4 who self-administered medical acupuncture and cupping therapy at home to full recovery.
Description
In detail, 37-year-old female anesthesiologist and board-certified medical acupuncturist working in a New York City COVID intensive care unit with no past medical history and no medication use presented with loss of smell and fatigue on April 17, 2020, diagnosis confirmed with COVID-19 nasal swab polymerase chain reaction positive. Pertinent negatives include no pulmonary disease, no cardiac disease, no renal insufficiency, and a zero pack year smoking history. Subsequently, pleuritic chest pain, shortness of breath with hypoxia, increased respiratory rate, dry cough, orthostatic hypotension (systolic blood pressures in the 80s), and headache developed 2 days later. Respiratory rate noted to be >30 with a pulse oximeter reading of 85% at rest and 92%–93% with painful recruitment breaths and self-proning.
No fevers or chills noted and given the very limited resources in New York City at the time, no further testing was pursued by the patient in light of her knowledge of proning and recruitment breaths and, importantly, the ability to self-increase oxygenation. Upon onset of anosmia, patient self-administered dry suction vacuum cup therapy (plastic, 1.5 in diameter) in the area of LU 1 bilaterally with significant cupping bruises after only a few minutes indicating both vascular compromise consistent with COVID-19 as well as from a Chinese medicine perspective, great underlying toxins.
Upon onset of pulmonary symptoms, patient self-administered acupuncture at points LU 2, LU 6, and ST 36 bilaterally × 30 minutes for 2 days as well as bleeding LU 11 bilaterally. GV14, Ding Chuan, and Chuan Xi, bilaterally needled on the second day of shortness of breath × 30 minutes. Seirin 0.20 × 30 mm needles were used for all points and inserted and manipulated to the point of De Qi as felt by the patient (varying from 1.5 to 2.5 cm depending on point). No moxibustion was used. Post-treatment, pleuritic chest pain was noted to be significantly diminished and breathing was subjectively easier (respiratory rate remained unchanged). Pulse oximetry also with noted improvement to the mid-90s while in the sitting position. No other pharmacologic treatment was used.
All pulmonary symptoms subjectively resolved after 2 days of treatment, with anosmia resolving (still present as of September 22, 2020). Antibodies noted to be present 3 weeks after most symptoms have resolved.
Results
With self-directed medical acupuncture as well as existing supportive treatment of recruitment breaths and self-proning, patient recovered successfully from likely severe4 COVID pneumonia within a week’s time without hospitalization.
Discussion
This report describes the application of medical acupuncture and cupping therapy as part of the supportive treatment for a frontline anesthesiologist working in New York City with COVID-19 pneumonia-related acute respiratory symptoms with success. As with all single case reports, there are limitations as this was a self-diagnosis of acute clinical pneumonia from confirmed COVID-19 infection in an otherwise healthy anesthesiologist with no previous risk factors. It is unknown if these results are reproducible in a spectrum of other patients, especially those who have pre-existing conditions. What is known is that there have been many cases of previously healthy individuals, such as the patient described, that went on to critical pneumonia requiring intubation and developing subsequent severe morbidity and mortality.
In this case, the patient was infected during a time and place when there were witnessed mass critical shortages in the health care system from personnel shortages to ventilator shortages to blood shortages to shortages of the oxygen supply itself. Self-directed acupuncture and cupping in this setting was a way in which this patient was able to try and circumvent a hospitalization.
The World Health Organization declared COVID-19 a pandemic on March 11, 2020. COVID-19 is highly contagious and most patients developing some element of respiratory symptoms. For New York City, in April it was reported that roughly 20% of those who presented to the hospital required ventilators.5 With no confirmed cure and no vaccine at the time of this writing, critical ventilator shortages and the potential for future recurrence of disease,6 it would make sense to investigate other supportive treatment protocols for COVID-19 patients.
Conclusions
TCM has been used for thousands of years and as expected has been used during past pandemics. Many studies have been conducted on Chinese herbal remedies with protocols published for various stages of the COVID-19 disease in the Chinese and European literature,7,8 but acupuncture studies with regard to COVID-19 are sparse. Acupuncture and cupping therapy are relatively easy to practice with minimal risks to the patients. There are specific lung meridian points that could be utilized to stimulate the respiratory system and ameliorate hypoxia and distress, such as LU 1 and LU 6, which are the Mu point and the Xi-Cleft point, both important and strong points for symptoms of acute respiratory problems such as dyspnea and pleuritic chest pain associated with COVID-19.9
One limitation is that practicing acupuncture and cupping would require direct patient contact, and full personal protection equipment might be indicated, which would make applying filiform needles to the correct points cumbersome and difficult. Although this could still be practiced, an alternative is conducting self-directed treatment or teaching qualified proceduralist through virtual teaching. These interventions could potentially optimize patients’ chance for recovery as well spare ventilators for others in need.